Laparoscopic Sleeve Gastrectomy (Gastric Sleeve)
Obesity is one of the most significant health problems of the modern world.
According to the WHO (World Health Organization), obesity is now considered a disease—not a cosmetic issue.
It is associated with numerous complications, including type 2 diabetes, hypertension, cardiovascular disease, and sleep apnoea.
When conservative treatment (diet, medication, etc.) fails, bariatric procedures offer effective solutions for significant weight loss and overall health improvement.
When should patients with obesity undergo surgery?
Surgery is indicated when the BMI (body mass index), expressed in kg/m², is:
- Greater than 34 kg/m² and accompanied by serious comorbidities such as type 2 diabetes, hypertension, cardiovascular disease, or sleep apnoea
- Greater than 40 kg/m² (an absolute indication for surgical treatment). In this case, obesity is defined as morbid obesity because the patient will soon develop complications related to excess weight
- Greater than 28 kg/m² in the presence of type 2 diabetes (metabolic surgery)
In these situations, surgical intervention is indicated.
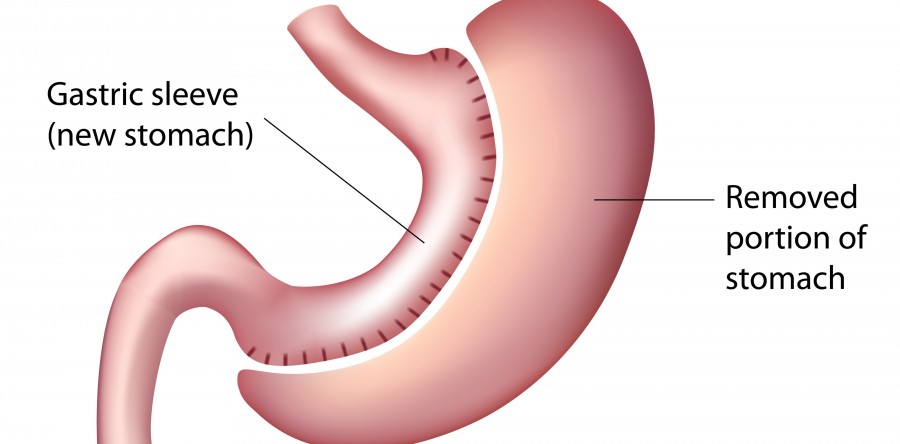
One of the most well-established surgical techniques since 2001 is the laparoscopic sleeve gastrectomy, commonly referred to by patients as the “gastric sleeve”.
The procedure restricts food intake (the stomach volume is surgically reduced), leading the patient to consume smaller quantities of food and therefore gradually lose body weight.
It also produces early satiety, meaning the patient feels full quickly and does not desire additional food.
As a result, the patient achieves substantial weight loss. This procedure is particularly suitable for individuals who typically consume large quantities of food (“big eaters”).
Before the operation, the patient undergoes a series of investigations, including gastroscopy, to identify known and unknown conditions.
A multidisciplinary medical team evaluates the patient (pulmonologist, cardiologist, gastroenterologist, the operating surgeon, etc.).
The operation is performed under general anesthesia.
Special laparoscopic instruments are used, and the procedure is carried out through 4–5 small abdominal incisions.
Hospital stay: strictly 3 to a maximum of 4 days (it should be noted that this is a form of gastrectomy).
From the day of surgery, the patient mobilizes immediately and is encouraged to walk. Pain is usually minimal.
The patient does not drink fluids or eat for 2–3 days but is hydrated with appropriate intravenous fluids.
Afterwards, the patient begins to drink liquids and later to eat, strictly following the written instructions provided by the surgeon.
These instructions MUST be followed EXACTLY to avoid complications.
Postoperative course
Patients:
• Begin to lose weight gradually, and by two years they approach their ideal body weight (the GOAL of the procedure)
• Are monitored until weight stabilizes, with blood tests to identify and correct vitamin deficiencies, anaemia, etc.
• May have their preoperative medications adjusted (antihypertensive, antidiabetic, cholesterol-lowering drugs). In some cases, discontinuation of these medications is recommended by the relevant specialist (an advantage of surgical treatment)
• May discontinue the use of CPAP for sleep apnoea if indicated (another advantage of surgical treatment)
• Receive short-term (1–2 months) enteral nutritional supplements to support the body’s nutritional needs. During this period, patients are trained in proper eating habits (chewing, swallowing small quantities, stopping when full)
• Are advised to begin physical activity—initially mild, then progressively increasing—contributing to faster weight loss and toning of the body
Postoperatively, ALL patients MUST be examined by their surgeon according to the follow-up protocol provided.