Colectomy is a major, but often necessary, surgical procedure involving the removal of a segment or, in some cases, the entirety of the large intestine (colon).
Although the prospect of such an operation may understandably raise questions or concerns, in practice it has proven life-saving for thousands of patients with benign or malignant colonic disease.
Advances in medical technology and operative techniques have made colectomy safer, more effective and associated with reduced postoperative burden for the patient.
Indications for Colectomy
The decision to perform a colectomy is never taken lightly.
It is based on clear clinical and radiological findings and constitutes a therapeutic intervention for conditions such as:
• Colorectal cancer: The most common indication. Surgical excision of the tumour is the first and most critical step in managing the disease.
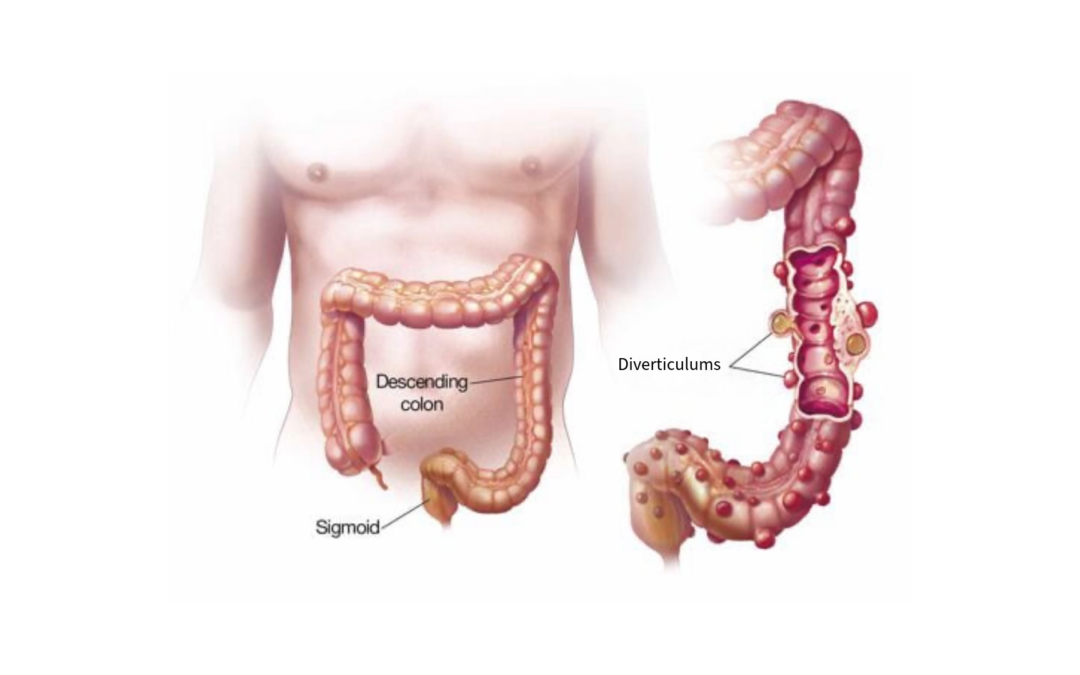
• Diverticulitis: Particularly in cases with recurrent episodes or complications such as abscess or perforation.
• Inflammatory bowel disease: In severe forms of ulcerative colitis or Crohn’s disease, colectomy may relieve chronic symptoms and frequent exacerbations.
• Polyposis syndromes: Such as familial adenomatous polyposis (FAP), where prophylactic colectomy is advised to prevent malignant transformation.
• Acute obstruction or perforation of the bowel: Situations requiring urgent surgical intervention.
Types of Colectomy
Colectomy is not a single, uniform operation. The type is tailored to the location of disease and the overall treatment plan:
• Right hemicolectomy: Removal of the caecum and ascending colon; typically used for malignancies or lesions on the right side of the colon.
• Left hemicolectomy: Targeting the descending colon for equivalent left-sided pathology.
• Transverse colectomy: Resection of the transverse colon, less common but necessary for isolated lesions.
• Sigmoid colectomy (sigmoidectomy): Very commonly performed for chronic diverticulitis or localised neoplasms of the sigmoid.
• Total colectomy: Indicated in severe inflammatory conditions or extensive malignancy; involves removal of the entire colon, with or without the rectum.
Preoperative Preparation
Proper preparation is essential for procedural success and patient safety:
• Colonoscopy is performed not only for diagnosis but to map the extent and location of disease.
• Radiological imaging (CT or MRI) is undertaken to assess intra-abdominal spread and potential complications.
• Routine blood tests and cardiology assessment ensure fitness for anaesthesia.
• Specific bowel preparation, including dietary modification and laxatives, reduces postoperative complications.
The Surgical Procedure
Colectomy may be performed using either an open (traditional) approach or a laparoscopic technique, the latter increasingly preferred due to its advantages: smaller incisions, reduced pain and faster recovery.
During the operation, the diseased portion of bowel is removed and, where feasible, an anastomosis is created—rejoining the healthy segments to restore continuity of the gastrointestinal tract.
In more complex or emergency settings, a stoma (colostomy or ileostomy) may be required, either temporarily or permanently, depending on the clinical situation.
Postoperative Recovery
Recovery varies among patients, but generally includes:
• Hospital stay of 4 to 10 days, depending on postoperative progress.
• Gradual reintroduction of diet, starting with liquids and progressing to light solid food.
• Early mobilisation, often from the first postoperative day, to prevent complications such as venous thrombosis or pneumonia.
• Stoma care education where applicable.
• Close medical monitoring for signs of infection, electrolyte disturbances or anastomotic complications.
Colectomy is a demanding yet highly effective procedure for patients with significant colonic disease.
With modern surgical methods, specialist perioperative management and active patient participation, outcomes are increasingly favourable and associated with substantial improvement in quality of life.