Gallbladder disease – whether we are talking about symptomatic gallstones, recurrent biliary colic, or inflammatory episodes—is a condition that does not promise improvement over time.
Once the gallbladder starts to malfunction, it keeps going downhill. That is why laparoscopic cholecystectomy has become the standard treatment, not out of habit but out of solid clinical experience.
The main reason is that a gallbladder with stones is an organ that “wakes up” whenever it feels like it. A patient may be fine for three months and then suddenly develop acute cholecystitis or even pancreatitis on a Saturday night, with fever and severe inflammation. Elective laparoscopic surgery in a calm setting prevents such scenarios.
Laparoscopy itself offers a clear advantage. Pain is less, mobilization is almost immediate, and hospital stay is short.
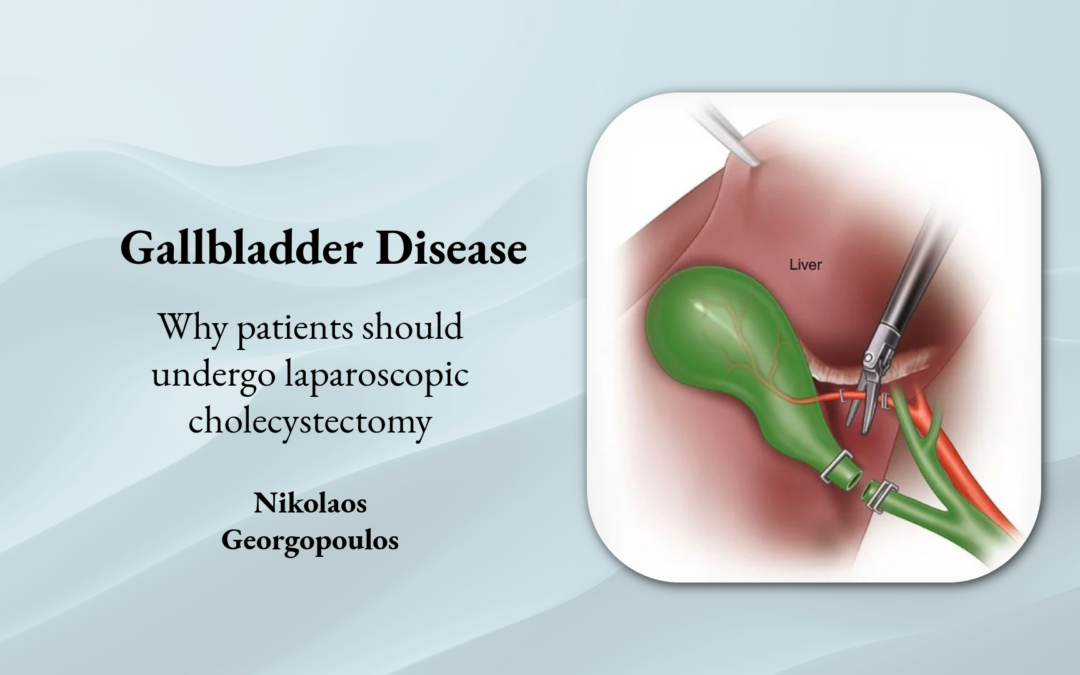
The liver and the biliary anatomy are seen much more clearly with camera magnification, which reduces the risk of injury when proper technique is used.
Postponement, on the other hand, hides dangers. Stones do not stay quiet. They can migrate and obstruct the common bile duct or the ampulla of Vater, leading to obstructive jaundice or pancreatitis—conditions that do not forgive delays.
A planned, calm operation is statistically far safer than surgery performed under the pressure of active inflammation.
There is also a practical point: open cholecystectomy rarely has a role when conditions are stable. The incision is larger, pain is greater, and complications such as wound infection and prolonged hospitalization increase.
Every symptomatic gallbladder is like a small, low-yield bomb. You do not know when it will go off, but you do know that it will. Laparoscopic cholecystectomy is simply the safest way to defuse it before it causes a much bigger problem.