Perianal fistulae are a common septic condition of the perianal region.
Symptoms:
• Seropurulent discharge (particularly when an abscess has drained spontaneously)
• Perianal pain
• Erythema and swelling of the perianal area
• Fever, often high and persistent, especially when the tract does not drain externally
Perianal fistulae frequently coexist with inflammatory bowel diseases such as Crohn’s disease.
Their aetiology is largely unknown. In many cases, fistula formation follows the drainage of a perianal abscess.
Treatment / Management:
Exclusively surgical, but utilising a minimally invasive technique.
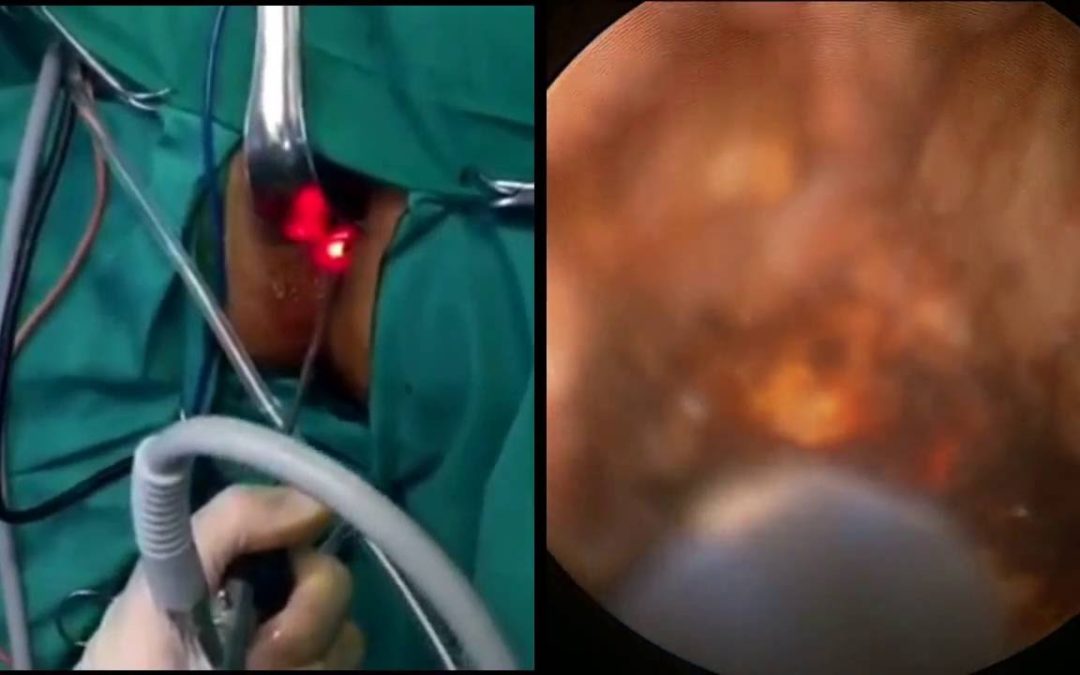
The method employs a dedicated endoscope: VAFT (Video-Assisted Fistula Treatment).
Under general anaesthesia (preferred):
a. Identification of the internal and external openings of the fistulous tract
b. Identification of the course of the tract using the endoscope
c. Instead of lay-open and drainage, the tract is destroyed from the external opening using diathermy. No large wound is created.
Particular attention must be paid to defining the relationship between the fistulous tract and the anal sphincter complex / pelvic floor musculature.
Only in this way can sphincter injury and subsequent faecal incontinence be avoided.
With this endoscopic technique, the sphincters are not affected, as no surgical division occurs.
Accurate and meticulous endoscopic destruction and drainage of the fistulous tract leads to good and rapid healing.
Assessment for perianal fistulae is best undertaken once an MRI of the region has first been performed.
This technique demonstrates very good outcomes in cases of recurrent fistulae or complex fistulous tracts.