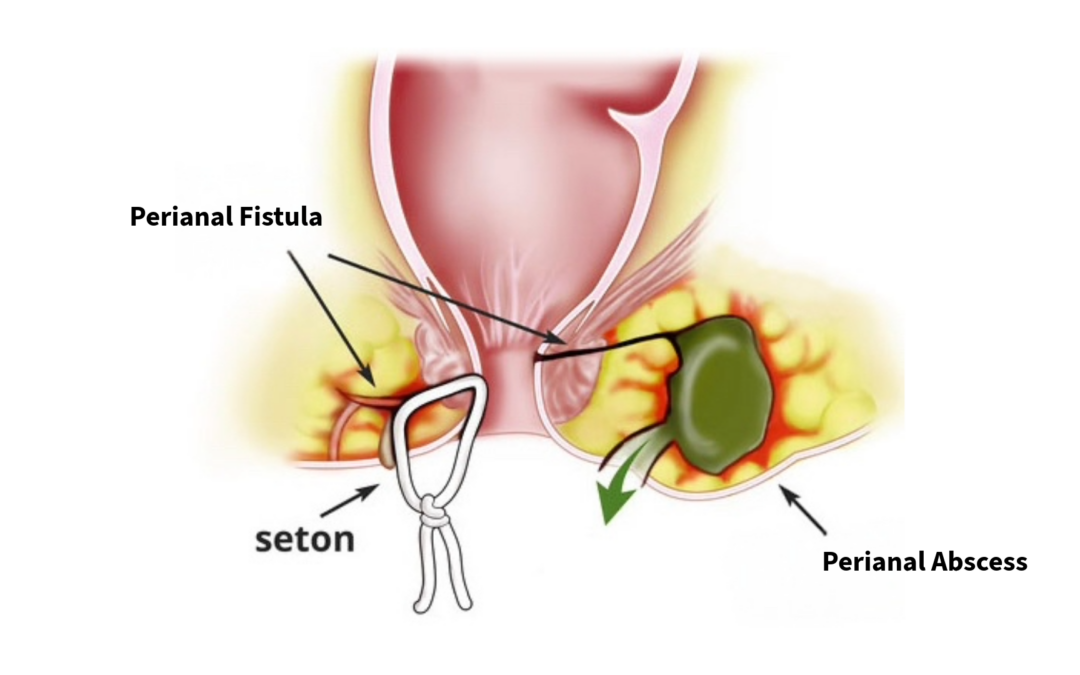
Perianal fistulae are a common septic condition of the perianal region.
Symptoms:
• Seropurulent discharge (particularly when an abscess has drained spontaneously)
• Perianal pain
• Erythema and swelling in the perianal area
• Fever, often high and persistent, especially when the tract does not drain externally
Perianal fistulae may coexist with inflammatory bowel diseases such as Crohn’s disease.
Their aetiology is largely unknown. In many cases, fistula formation follows the drainage of a perianal abscess.
Treatment / Management: Surgical only.
Under regional or, preferably, general anaesthesia, the following steps are undertaken:
a. Identification of the course of the fistulous tract
b. Identification of the internal and external openings
c. Lay-open and drainage of the fistulous tract, allowing healing by secondary intention.
In many cases, seton placement is required when the tract traverses the external anal sphincter.
Particular attention must be paid to accurately determining the relationship between the fistulous tract and the anal sphincter complex / pelvic floor muscles.
This is essential to avoid sphincter injury and subsequent faecal incontinence.
Adequate and thorough drainage is a prerequisite for successful healing.
It is advisable to avoid simultaneous exploration for fistulous tracts during abscess drainage and to avoid concurrent fistula treatment, in order to minimise the risk of injury to healthy tissues.
Evaluation for perianal fistulae is best performed subsequently, once an MRI of the region has been obtained.